Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2024 Edition) 1
Traditional thermal and cryoablation techniques should be used with caution in hepatocellular carcinoma adjacent to the hepatic hilum or near the first- and second-order bile ducts, and a safety distance of at least **>5 mm** from adjacent critical structures is recommended.
Ablation therapy should be used with caution for hepatocellular carcinoma adjacent to the hepatic hilum or near the first- and second-order bile ducts, to avoid complications such as bile duct injury.Percutaneous ethanol injection (PEI) is a relatively safe option, or ablation may be combined with PEI. If thermal ablation is used, a sufficient safety margin (at least >5 mm) must be maintained between the tumor and the first- and second-order bile ducts, and safe ablation parameters (low power, short duration, intermittent radiation) should be adopted. Temperature monitoring is recommended for ablation devices with this capability.
Expert consensus on the standard of radiofrequency ablation therapy for liver cancer
Complications after radiofrequency ablation of liver cancer may include post ablation syndrome, infection, gastrointestinal bleeding, intra-abdominal bleeding, tumor implantation, liver failure, adjacent organ damage, etc.
1. Post ablation syndrome: mainly manifested as fever, pain, etc., rare cases include hematuria, chills, etc., the specific cause is unknown. The main treatment includes strengthening postoperative monitoring, intravenous infusion, pain relief, symptomatic treatment, and regular liver and kidney function testing.
2. Infection: Mainly includes liver abscess, puncture site infection, etc. Prevention: Strict aseptic operation, antibiotics can be used to prevent infection after surgery.
3. Gastrointestinal bleeding: The main cause is bleeding from varicose veins in the lower esophagus or bleeding from stress ulcers. Prevention and treatment: For patients with severe portal hypertension, preoperative management of portal hypertension is recommended; Routine use of antacids after surgery to prevent stress ulcer bleeding. Post bleeding treatment: vital signs should be checked, fasting should be avoided, active volume expansion, intravenous infusion, hemostasis, blood transfusion, acid production, pressure boosting, etc. Endoscopic hemostasis should be performed if necessary.
4. Abdominal bleeding: Clinical manifestations depend on the amount of bleeding. Minor bleeding without obvious symptoms. When there is a large amount of bleeding, there is often bloating and abdominal pain, and in severe cases, cold sweat, decreased blood pressure, and shock symptoms. The main reason is that the tumor is relatively superficial and ruptures after puncture; Or the patient may have poor coagulation function and bleeding at the liver puncture site. Prevention: Strictly grasp the indications, and for patients with poor coagulation function in cirrhosis, correct them before treatment; For superficial lesions, it is best to use laparoscopy or open abdominal visualization. During percutaneous radiofrequency therapy, the number of punctures should be minimized, needle ablation should be performed, and ultrasound or CT scans should be performed again after ablation to rule out the presence of tumor rupture, bleeding, and other symptoms. Treatment: Check vital signs, actively expand volume, administer intravenous fluids, stop bleeding, transfuse blood, increase blood pressure, etc. If necessary, perform surgical exploration to stop bleeding.
5. Tumor implantation: mainly caused by repeated punctures. Prevention: Puncture should be accurately located to avoid repeated punctures; If the needle is inserted too deeply, the electrode needle should not be directly retracted, but should be repositioned after in-situ ablation.
6. Liver failure: The main reason is severe liver cirrhosis and poor liver function before treatment; Or serious complications may occur (such as infection, bleeding, etc.). Prevention and treatment: Strictly control the indications, and cases with Child Pugh C liver function, large ascites, severe jaundice, etc. are all contraindications; After surgery, pay attention to preventing the occurrence of other complications, preventing infections, and actively treating liver protection. 7. Adjacent organ damage: When the tumor is located near the gallbladder, gastrointestinal tract, bile duct, diaphragm, or in the first porta hepatis area, subcapsular area, etc., percutaneous ablation treatment through the puncture pathway may easily cause thermal damage to adjacent organs or vessels. For tumors in these areas, laparoscopic or open surgery under direct visualization should be used as much as possible for radiofrequency ablation treatment, and adjacent organs should be isolated and protected.
Chinese expert consensus on CT guided thermal ablation therapy for primary liver cancer (2023 edition)
Traditional thermal ablation reduces tissue temperature due to blood flow near large blood vessels, which may carry away heat and lead to incomplete ablation of tumor tissue near blood vessels.
Heat sink effect: When a tumor is ablated, the flow of blood near large blood vessels (usually>3mm in diameter) reduces the temperature of the tissue, which may take away heat and cause incomplete ablation of the tumor tissue near the blood vessels, adversely affecting the ablation results.
Expert consensus on the standard of radiofrequency ablation therapy for liver cancer
Tumors located near the gallbladder, gastrointestinal tract, bile duct, diaphragm, or in the first porta hepatis area or under the liver capsule are all considered high-risk areas. Radiofrequency ablation therapy for tumors in these areas carries risks of thermal damage to adjacent organs or vessels, tumor rupture, and bleeding.
Radiofrequency ablation of tumors in high-risk areas: Tumors located near the gallbladder, gastrointestinal tract, bile duct, diaphragm, or in the porta hepatis area or under the liver capsule are considered high-risk areas. Radiofrequency ablation treatment for tumors in these areas carries risks of thermal damage to adjacent organs or veins, tumor rupture, bleeding, etc., so special care should be taken. For tumors in high-risk areas, laparoscopic or open surgery under direct visualization should be used for ablation treatment as much as possible to isolate and protect adjacent organs. There are also reports of radiofrequency ablation treatment under artificial pleural effusion, artificial ascites, or special techniques such as lifting.
Guidelines for Diagnosis and Treatment of Primary Liver Cancer (2024 Edition)
Ablation therapy is currently considered one of the curative methods for treating liver cancer besides surgical resection, with the characteristics of minimal impact on liver function, minimal trauma, and definite therapeutic effect.
Ablation therapy: Currently, ablation therapy is considered a curative treatment for small liver cancer in addition to surgical resection. Ablation therapy has the characteristics of minimal impact on liver function, minimal trauma, and definite efficacy. In some early liver cancer patients, it can achieve similar therapeutic effects as surgical resection.
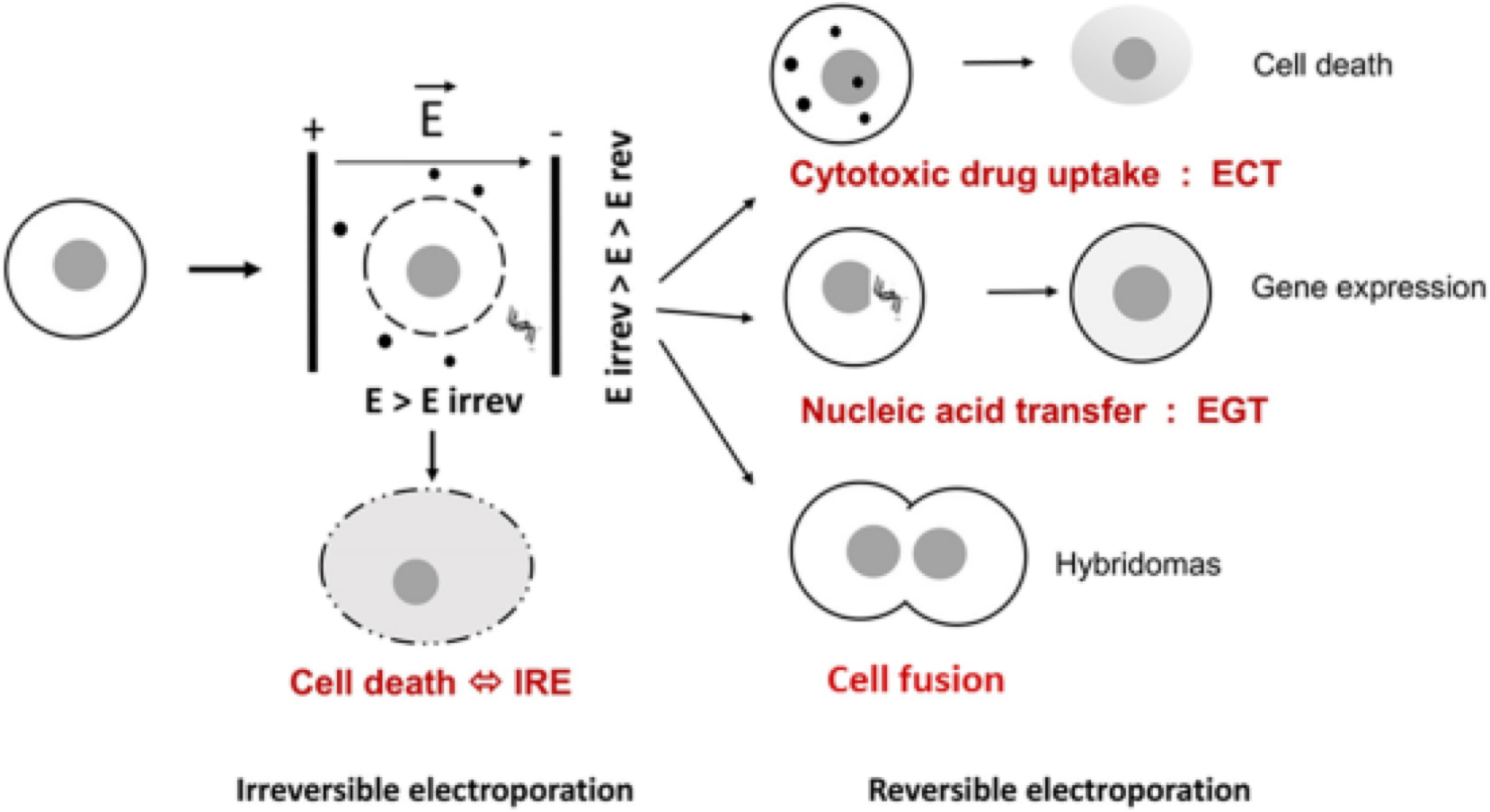
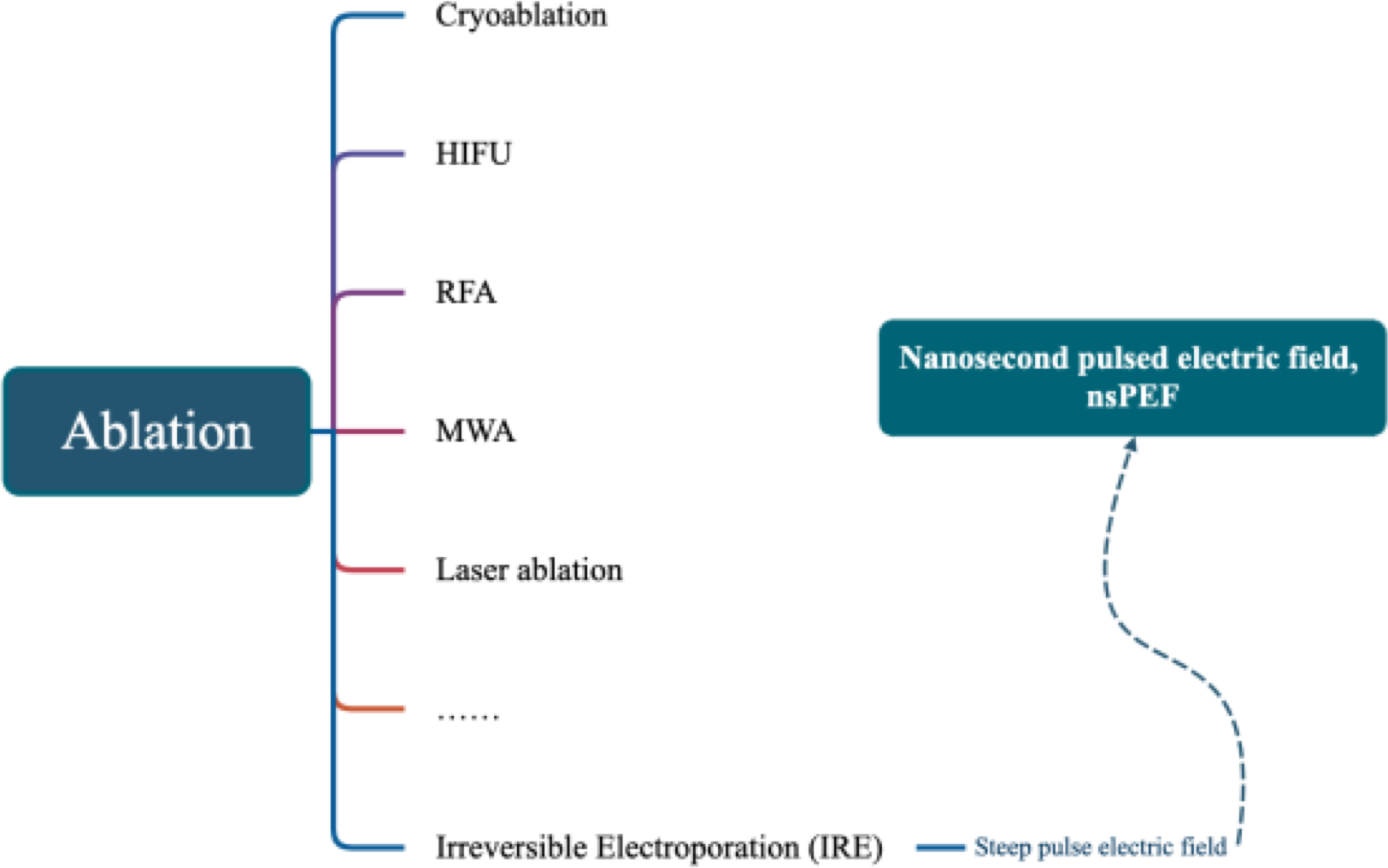
Clinical practice guidelines for ultrasound-guided irreversible electroporation ablation therapy for liver cancer (2023 edition)
Include important structures adjacent to the tumor, such as the porta hepatis, blood vessels, bile ducts, diaphragm, or gastrointestinal tract, as indications.
Indications and Contraindications - Indications: Malignant liver tumors diagnosed clinically or pathologically, with a single diameter ≤ 5cm; or multiple tumors (≤ 3 in number), with a maximum diameter ≤ 32 cm. Tumors are located adjacent to important structures such as the porta hepatis, blood vessels, bile ducts, diaphragm, or gastrointestinal tract; 3 liver function grades Child Pugh A/B; 4. For single tumors with a diameter greater than 5cm or multiple tumors with a diameter greater than 3cm that cannot be surgically removed, palliative ablation or combination with other treatment methods can be used; The expected survival period is over 3 months, and the Karnofsky functional status score is>50.